Vendor Contracts After Buying a Practice: Transfer or Renegotiate
Co-Founder, Minty Dental

In Summary
- Vendor contracts don't automatically transfer with an asset purchase—assignment clauses and change-of-control provisions in each contract determine whether you need vendor consent, face renegotiation, or inherit terms as-is
- The transition period creates negotiating leverage that disappears fast: vendors want to retain the account, and you have fresh perspective on pricing the seller accepted years ago without review
- Pull six months of bank statements during due diligence to find contracts the seller forgot—software subscriptions, equipment maintenance, and services that auto-renew quietly but weren't disclosed
- A three-bucket framework helps prioritize: auto-transferable contracts (minimal attention), consent-required (proactive outreach), and renegotiation targets (unfavorable terms or pricing above market)
- Most buyers treat vendor contracts as administrative paperwork when they're actually a negotiating window—practices that renegotiate supply, lab, and equipment contracts in the first 90 days capture savings that compound for years
Most Vendor Contracts Don't Automatically Transfer—And That's Both Risk and Opportunity
When you sign an asset purchase agreement, the legal document typically lists vendor contracts as part of what you're acquiring. That language creates the impression that continuity is automatic—that the lab relationship, supply agreements, and software subscriptions simply roll forward under new ownership. In most cases, that's not how it works.

Whether a contract can be transferred depends on the contract's assignment language, not the purchase agreement. Some vendor contracts prohibit assignment entirely without written consent. Others allow assignment but require advance notice or approval. A small subset transfer automatically with no restrictions. The purchase agreement can say you're buying the contracts, but if the contract itself says "non-assignable," you're starting from zero with that vendor unless they agree to the transfer.
Even if you don't formally assign a contract, a change in practice ownership can trigger termination rights or price adjustments. Many vendor agreements include change-of-control clauses that treat an ownership transition as a material event—giving the vendor the option to exit the relationship, renegotiate terms, or adjust pricing. You can inherit a contract without legally assigning it and still face disruption if the vendor exercises those rights.
Where buyers get burned is assuming that because a contract appears in the asset list, it's locked in. You find out 30 days post-closing that the lab requires a new agreement, the supply distributor wants updated credit terms, or the software vendor is raising fees because the original contract was tied to the seller's entity. By then, you're operationally dependent and negotiating from a weaker position.
The transition period creates leverage that disappears quickly. Vendors want to retain the account—they've invested in the relationship, and losing a practice means lost revenue and replacement costs. You're coming in with fresh perspective on pricing the seller accepted years ago, often without revisiting terms or comparing alternatives. That combination—vendor retention risk plus your willingness to evaluate competitors—is negotiating power, but only if you use it before closing or within the first 60–90 days.
A practical framework for categorizing contracts during due diligence:
-
Auto-transferable: Contracts with no assignment restrictions or change-of-control provisions. These transfer cleanly and require minimal attention beyond confirming the vendor has updated records.
-
Consent-required: Contracts that explicitly require vendor approval for assignment or that include change-of-control language. These need proactive outreach during due diligence to secure written consent and confirm terms remain unchanged.
-
Renegotiation targets: Contracts with unfavorable pricing, outdated terms, or vendors you'd consider replacing. These are opportunities to negotiate better rates, updated service levels, or contract structures that fit your operating model—not the seller's.
Most buyers spend due diligence verifying that contracts exist and then move on. The higher-value exercise is sorting contracts into these three buckets and building a transition plan that protects continuity while capturing cost savings. Outstanding vendor contracts represent one of several liability categories that can surface post-closing if not properly addressed during review. One area where this applies beyond vendor agreements is digital assets like phone numbers and websites, where transfer mechanics and ownership structures often require separate attention during closing.
The risk isn't that vendor contracts are complicated—it's that they're easy to treat as administrative paperwork when they're actually a negotiating window that closes fast.
Which Vendor Contracts Require Review During Due Diligence
The contract register most sellers provide during due diligence is incomplete. Not because they're hiding anything—most practice owners genuinely don't remember every recurring vendor relationship they've established over years of operation. Software subscriptions auto-renew quietly. Equipment maintenance agreements get bundled into invoices. Lab relationships operate on handshake terms with no formal contract on file.
One step that catches what the contract register misses: pull six months of bank statements and check registers, then cross-reference every recurring payment against the disclosed vendor list. You'll find contracts the seller forgot, services that renewed automatically, and subscriptions that haven't been used in years but are still being paid.
Dental Supply Contracts
What to review: Pricing tiers, volume commitments, minimum purchase requirements, and whether the seller negotiated group purchasing organization (GPO) discounts that transfer with the practice. Many supply agreements include tiered pricing based on annual spend—if the seller qualified for a volume discount you won't hit in year one, your per-unit costs could jump 15–20% without warning.
Why it matters: Supply costs typically run 5–7% of collections, and pricing structures vary widely between distributors. Some sellers lock in favorable terms through GPO memberships or multi-year commitments; others accept list pricing and never revisit it.
Red flags: Exclusive purchasing requirements that limit your ability to source competitively, contracts that penalize you for switching distributors mid-term, or pricing significantly above market rates for comparable practices in your region.
Lab Agreements
What to review: Turnaround guarantees, pricing per case type (crown and bridge, implants, removable), and whether the contract is exclusive or allows you to use multiple labs. Some lab agreements include quality guarantees or remake policies that protect you if cases come back incorrectly; others put all risk on the practice.
Why it matters: Lab costs are one of the largest variable expenses in restorative-focused practices, and pricing can vary 30–40% between labs for identical work. If the seller built a relationship with a high-quality lab at competitive rates, that's value worth preserving. If they're overpaying out of convenience or loyalty, the transition is your window to evaluate alternatives.
Red flags: Exclusive agreements that prevent you from sending cases elsewhere, pricing above regional benchmarks, or turnaround times that don't align with your clinical workflow.
Equipment Leases and Maintenance Contracts
What to review: Which equipment is leased versus owned outright, lease buyout terms, and whether maintenance agreements are bundled with the lease or contracted separately. Many sellers assume equipment is included in the sale when it's actually leased.
Why it matters: Equipment leases often include personal guarantees from the seller, which don't automatically transfer to you. If the lease requires vendor consent for assignment and the vendor declines, you may need to negotiate a new lease at current rates—or buy out the remaining term at a premium.
Red flags: Leases with high buyout costs relative to equipment age, maintenance contracts that auto-renew with 90-day notice periods, or bundled agreements where you're paying for coverage on equipment you plan to replace.
Software and EMR Systems
What to review: License transfer procedures, data migration costs, per-provider or per-location pricing, and whether the contract includes support and updates or charges separately. Many practice management systems tie pricing to the number of providers or locations—if you're adding associates or opening a second site, costs can increase substantially.
Why it matters: Software transitions are among the highest-risk vendor changes because they affect every operational workflow in the practice. If the seller's EMR contract doesn't transfer cleanly, you're either negotiating a new agreement under time pressure or migrating to a different system entirely—both of which disrupt scheduling, billing, and patient communication during your first months of ownership.
Red flags: Contracts that charge per-provider and increase fees automatically when you add staff, data migration fees that weren't disclosed upfront, or systems where the seller has unpaid balances or unresolved support issues.
Waste Management and Specialized Services
What to review: Medical waste disposal contracts, answering services, IT support agreements, and payroll processing vendors. These are the contracts most likely to be missing from the seller's disclosure because they operate in the background—monthly invoices get paid automatically, and no one thinks to list them as "contracts" during due diligence.
Why it matters: Waste management contracts often include auto-renewal clauses and early termination penalties. If you're planning to switch vendors or renegotiate pricing, you need to know the notice period and whether the contract locks you in for another 12–24 months.
Red flags: Contracts with 90-day auto-renewal windows you've already missed, early termination fees that exceed the cost of riding out the contract term, or vendors providing services the practice no longer needs but continues paying for out of inertia.
Building the Contract Inventory
Request the complete contract register during due diligence, but don't stop there. Cross-reference it against six months of bank statements and check registers to identify every recurring vendor payment. For each contract, note the renewal date, notice period for termination, and whether assignment requires vendor consent. Due diligence reviews typically span two to four weeks, and incomplete vendor documentation is one of the most common causes of delays.
This inventory becomes your roadmap for the first 90 days—showing you which contracts need immediate attention, which can wait until renewal, and where cost savings are sitting unclaimed. Where buyers lose money isn't in the contracts they review—it's in the ones they don't know exist until the first invoice arrives post-closing.
How to Secure Vendor Consent and Avoid Post-Closing Disruptions
The mechanics of vendor transfer approvals are straightforward—notify the vendor, provide new entity details, wait for confirmation. Where buyers run into trouble is timing the process poorly or treating vendor consent as a formality when it's actually a negotiation.
When to initiate vendor notifications: Start after the LOI is signed but early enough to complete approvals before closing. Some vendors process transfers in 7–10 business days; others take 30–60 days, particularly if they require credit applications or committee approvals. For critical vendors—your primary supply distributor, lab, practice management software—initiate contact within the first week after LOI execution.
Who handles vendor outreach: In most transitions, the seller makes initial contact to introduce you and signal their support for the transfer. This preserves the existing relationship and reduces vendor resistance. You or your attorney then follow up with the formal transfer request, including all required documentation. For vendors where you're planning to renegotiate terms, consider handling outreach directly from the start—this frames the conversation as a new business relationship rather than a simple administrative transfer.
What vendors typically require: Most vendors need your new entity's legal name, tax ID (EIN), and a completed credit application. Some request personal guarantees from the new owner, particularly for equipment leases or high-volume supply agreements. Others want proof of professional liability insurance or state licensure verification.
When vendors use transfer approval as leverage: A subset of vendors will respond to your transfer request by proposing updated pricing, new contract terms, or additional fees. This happens most often with software vendors, equipment lessors, and supply distributors where the seller negotiated favorable rates years ago.
One protection many buyers overlook is comparing proposed rates to current market benchmarks before accepting the increase. Vendors expect some pushback—they're testing whether you'll accept the new terms without question. Pull quotes from two competing vendors for the same service, then return to the original vendor with data showing their proposed pricing is 15–20% above market. In most cases, they'll adjust closer to the original terms because they want to retain the account.
Protecting yourself with closing conditions: For vendors that are operationally critical—your EMR system, primary lab, or supply distributor—include transfer approval as a closing condition in the purchase agreement. This language protects you if a vendor refuses consent or demands terms that fundamentally change the economics of the deal.
What to do when a vendor refuses to transfer: Vendor refusals are rare, but they happen—usually with equipment lessors who want to write a new lease at current rates or software vendors who see the ownership change as an opportunity to upsell additional modules. When this occurs, evaluate whether you can switch providers without disrupting patient care, and whether the cost of switching exceeds the cost of accepting the vendor's new terms.
For non-critical vendors, switching is often the better financial decision. For critical systems—particularly your EMR or phone system—the disruption cost may justify accepting revised terms in the short term while you plan a longer-term migration.
Managing the approval timeline: Track each vendor's approval status in a spreadsheet with columns for vendor name, contact date, required documentation, approval status, and follow-up date. Most vendors respond within two weeks if you've provided complete information; if you haven't heard back after 10 business days, follow up directly.
The transition period is short, and vendor dependencies are real. Practices that secure consent early and treat the process as a negotiation—not a formality—enter ownership with continuity protected and costs controlled. Those that wait until the last minute or accept vendor terms without question pay for that approach in higher costs and weaker positioning for years after closing.
Where to Renegotiate and What Leverage You Actually Have
The assumption most buyers carry into closing is that inherited contracts are fixed—that the pricing the seller accepted is the pricing you'll pay, at least until the next renewal cycle. That assumption costs practices tens of thousands annually in unnecessary vendor expenses. Most vendor contracts are negotiable at transition, and the pricing you're inheriting often hasn't been reviewed in years.
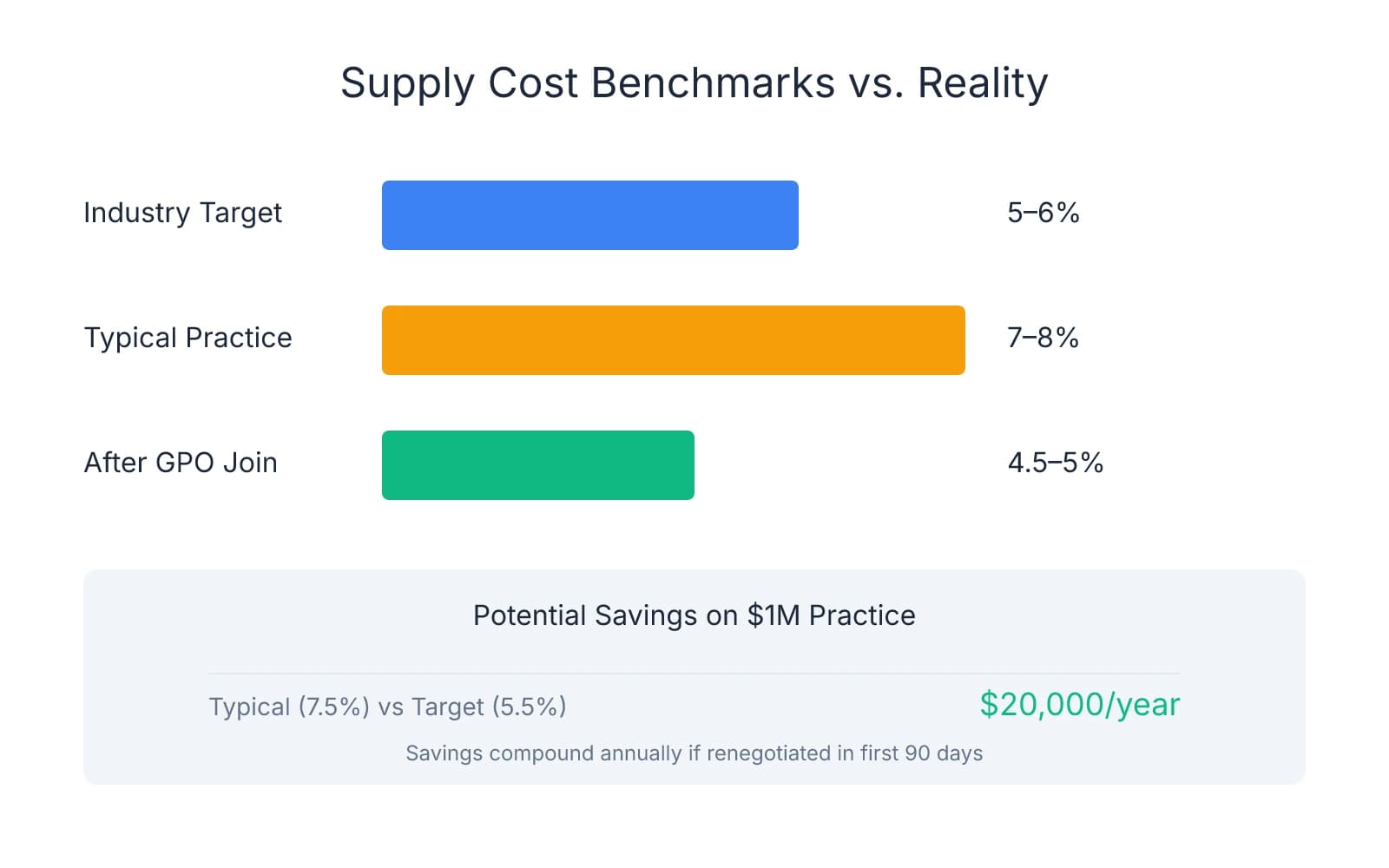
Dental supply contracts sit at the top of the renegotiation target list. Industry benchmarks suggest supply costs should run 5–6% of collections, but many practices pay 7–8% because the seller locked in pricing three to five years ago and never revisited it. Supply distributors expect negotiation—their sales reps have discretion to adjust pricing, particularly when a new owner signals they're evaluating alternatives.
One approach that creates immediate leverage: request a line-item pricing comparison from two competing distributors for your top 50 supply items, then bring that data back to the incumbent vendor. In most cases, they'll match or beat competitive pricing to retain the account, because the cost of losing you exceeds the margin they give up by lowering rates.
Lab contracts offer similar negotiation potential if you can demonstrate volume or if competitive labs serve your area. Before accepting the seller's lab pricing, request quotes from two alternative labs for your top 10 case types—crown and bridge, implants, dentures, and any specialized work your practice handles regularly. Present those comparisons to the current lab with a straightforward question: can you match these rates to keep our business? Many labs will adjust pricing 10–15% rather than lose a consistent volume account.
Software and EMR contracts have less pricing flexibility, but terms are negotiable. Most practice management systems operate on fixed per-provider or per-location licensing models, and vendors rarely discount the base subscription cost. Where you can negotiate is on support, training, and additional licenses. If you're committing to a multi-year renewal, request enhanced support or additional training sessions at no extra cost.
Group purchasing organizations (GPOs) provide leverage that independent practices can't achieve alone. GPOs aggregate purchasing volume across hundreds of practices to negotiate pre-negotiated pricing with major vendors—typically delivering 15–30% savings on supplies, lab work, and equipment compared to individual practice pricing. Practices that join GPOs within the first 90 days of ownership capture savings immediately, while those that wait often continue paying inherited pricing for months before realizing better options existed.
Timing major renegotiations for 60–90 days after closing gives you data to negotiate from. Walking into vendor conversations during due diligence with assumptions about usage patterns puts you at a disadvantage—you're guessing at volume, estimating needs, and negotiating without leverage. Waiting 60–90 days lets you review actual supply orders, lab case volume, and software utilization before approaching vendors.
A framework for identifying which contracts to renegotiate first:
- Contracts the seller signed years ago without recent review — these often carry outdated pricing that vendors will adjust if challenged
- Vendors with competitive alternatives in your market — leverage only exists when you can credibly walk away
- Contracts with pricing above industry benchmarks — if your supply costs exceed 6% of collections or your lab pricing sits in the top quartile for your region, renegotiation should be immediate
The best leverage is credible alternatives. Vendors adjust pricing when they believe you're evaluating competitors and willing to switch if terms don't improve. That means doing the research before initiating renegotiation—pulling quotes, understanding market rates, and identifying which vendors you'd actually move to if negotiations fail.
Where buyers leave money on the table is assuming they must accept inherited contracts because switching vendors feels disruptive. Vendors expect negotiation at ownership transitions—they've built margin into their pricing specifically to accommodate it. The question isn't whether you should renegotiate; it's whether you'll do it strategically in the first 90 days when you have leverage, or wait until you're operationally dependent and negotiating from a weaker position.
The transition period creates a narrow window where vendors want to retain your business and you have fresh perspective on pricing the seller accepted without question. That combination doesn't last—use it while it exists, or pay the cost of inherited contracts for years after closing. For practices evaluating where else to optimize costs in year one, similar strategic thinking applies to decisions around staff compensation adjustments and marketing budget allocation—all areas where new ownership creates opportunity to reset baselines rather than inheriting the seller's approach by default.
Sources & References
The data and claims in this article are drawn from the following sources. We prioritize government data, peer-reviewed research, and established industry publications to ensure accuracy.
- Red Flags in Dental Practice Purchase Agreements— mahandentallaw.com
- How Long Does It Take to Purchase a Dental Practice?— polishedlegal.com
- Dental Practice Post-Closing Obligations— mahandentallaw.com
Ready to navigate vendor contracts smoothly?
Vendor contract management is complex after a practice acquisition. Minty Plus provides expert guidance through contract transfers, renegotiations, and change-of-control issues to protect your investment.


