When the Seller Won't Leave: Managing Interference After Closing
Co-Founder, Minty Dental

In Summary
- Most transition agreements specify duration and pay but leave the seller's decision-making authority undefined — creating confusion about who actually runs the practice
- Staff continue seeking the seller's approval on operations even after closing because symbolic authority (who people defer to) matters more than legal ownership in the first 90 days
- Three seller patterns drive interference: the shadow operator still acting like owner, the reluctant retiree not ready to leave, and the helpful mentor who doesn't recognize when support becomes destabilization
- Tight agreements define the role as patient introductions only, script the seller's redirects to staff questions, and include early termination language if boundaries are violated
The Transition Period Creates a Power Vacuum Unless You Define It First
The purchase agreement closes. You wire the funds. The practice is legally yours. Yet three weeks later, your hygienist still asks the seller whether she can order supplies, your front desk checks with him before confirming schedule changes, and patients ask when "Dr. [Seller]" will be back full-time.
This isn't a failure of goodwill — it's a failure of structure. Most transition agreements specify duration and compensation but leave the seller's actual role undefined. The contract says they'll "assist with patient introductions," but doesn't clarify who makes the final call when a patient reschedules, when staff request time off, or when a vendor needs contract approval. That ambiguity creates a power vacuum, and vacuums get filled by whoever was there first.
Three Archetypes That Create Interference
The shadow operator technically handed over the keys but still walks the hallway like they own it. They're the first person staff approach with questions. They override your decisions in casual conversations. They reassure patients that "everything will stay the same" — which sounds comforting until you realize it means you aren't allowed to change anything.
The reluctant retiree agreed to sell because the timing made financial sense but wasn't emotionally ready to leave. Sellers who lack a clear post-sale plan often struggle to let go, and that ambivalence shows up as lingering involvement. They extend the transition informally, offering to "help out" beyond the contracted window. Staff interpret this as the seller's lack of confidence in you.
The overstaying mentor genuinely wants to help but doesn't recognize when their presence shifts from supportive to destabilizing. They're still checking in with staff, weighing in on clinical decisions, positioning themselves as institutional memory. The problem isn't malice — it's that their symbolic authority hasn't transferred, and every day they remain visible reinforces the old power structure.
Symbolic Power Trumps Legal Ownership
In the first 90 days, what matters isn't who owns the practice on paper — it's who staff and patients believe is in charge. Employees take cues from symbolic gestures: whose name is on the door, who the seller defers to in front of the team, whose decisions get quietly overruled in side conversations. If the seller continues behaving like the final decision-maker — even informally — the team treats you like interim manager, not owner.
Watch how the seller introduces you to patients. If they say "Dr. [Buyer] will be helping out while I step back," patients hear you're the backup. If they say "Dr. [Buyer] is taking over, and I'm staying briefly to ensure a smooth transition," the power structure is clear. The difference is subtle but determines whether patients see you as new authority or the seller's temporary replacement.
The fix isn't hoping the seller naturally steps back. It's defining their role with enough specificity that there's no ambiguity about who makes decisions once the deal closes. That structure needs negotiation before you sign, not after you realize the seller is still running the practice from the hallway.
What Belongs in a Transition Agreement That Actually Protects You
The transition agreement most buyers sign contains three numbers — duration, compensation, days per week — and almost nothing about what the seller can actually do. That gap is where interference lives. A well-structured agreement doesn't just specify how long the seller stays — it defines their role boundaries so narrowly there's no room to act like they still run the practice.
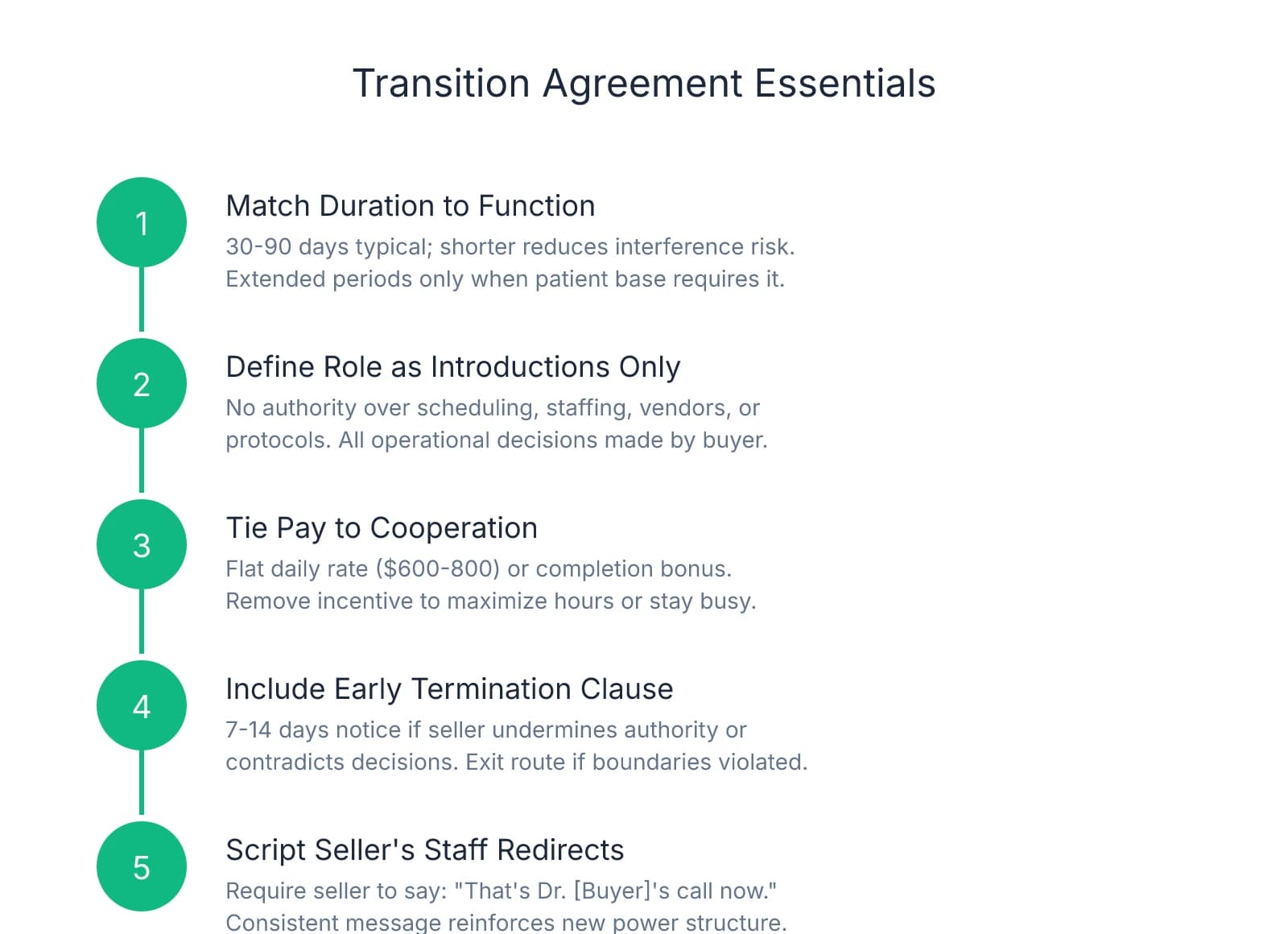
Match Duration to Function, Not Sentiment
Transition periods typically range from 30 to 90 days, with the shorter end sufficient when staff is stable and the patient base established. The risk isn't that 30 days is too short — it's that six months is too long. Extended transitions increase the likelihood the seller drifts from introductions into operational input, especially if their role isn't tightly defined.
One question worth asking during negotiation: does this practice actually need 90 days of seller presence, or does the seller just want 90 days of income? If the patient schedule is full and staff has been there for years, 30–45 days is often enough. Longer periods make sense when the practice has high patient turnover, the buyer is relocating from out of state, or the seller has a specialized patient base requiring clinical handoffs. Otherwise, a shorter window reduces interference risk without sacrificing continuity.
Define the Role as Patient Introductions Only
Most transition agreements are too broad: "The seller will assist with patient introductions and provide clinical support as needed." That phrasing gives the seller implicit permission to weigh in on anything they consider "support" — which, in practice, means everything.
What works better: "The seller's role is limited to introducing patients during scheduled appointments and completing work in progress. The seller has no authority over scheduling, staffing decisions, vendor contracts, or clinical protocols. All operational decisions are made solely by the buyer." That's not hostile — it's clarity. The seller can still be helpful within those boundaries but can't override your decisions or position themselves as parallel authority.
One protection many buyers overlook is a clause requiring the seller to defer to the buyer's decisions in front of staff and patients. Without that language, you'll end up in situations where the seller contradicts your clinical recommendations during patient conversations or tells your front desk to ignore a policy change you just implemented.
Tie Compensation to Cooperation, Not Production
Most transition agreements pay the seller a percentage of their production during the transition — usually the same rate they'd pay an associate. That creates a problem: the seller's financial incentive is to keep seeing patients and generating revenue, not to step back and let you take over.
A better model ties compensation to cooperation rather than output. Some buyers negotiate a flat daily rate — $600–$800 per scheduled day, regardless of production — which removes the financial incentive to maximize clinical hours. Others structure it as a completion bonus: the seller receives a lump sum at the end if they fulfill obligations and exit on schedule. Transition agreements can include performance-based elements that reward smooth handoffs rather than prolonged involvement.
The seller's compensation shouldn't depend on them remaining indispensable. If they're paid more for staying busy, they'll stay busy. If they're paid for showing up, introducing patients, and stepping back on time, that's what they'll do.
Build in an Early Termination Clause
Even with tight language, some sellers push boundaries. That's why the agreement needs an exit mechanism that doesn't require mutual consent. A standard early termination clause allows the buyer to end the transition with 7–14 days' notice if the seller undermines authority, contradicts buyer decisions in front of staff, or otherwise interferes with operations.
This isn't about creating contentious relationships — it's about ensuring you're not locked into 90 days of interference because the contract has no escape route. Most sellers never trigger the clause, but knowing it exists changes the power dynamic. The seller understands cooperation isn't optional, and you're not stuck hoping they'll voluntarily step back.
What to Do If You're Already Past Closing
If you're reading this after the deal closed and the agreement is vague, you're not without options. Document expectations in writing, even retroactively. Send the seller an email: "To make sure we're aligned, here's how I understand your role over the next 60 days: patient introductions during scheduled appointments, no involvement in staffing or operational decisions, and a clean handoff by [date]. Let me know if you see it differently."
That email doesn't rewrite the contract, but it creates a record of expectations. If the seller continues interfering after you've clarified boundaries in writing, you have documentation to support an early exit or, if necessary, a conversation with your attorney about whether the seller is breaching the agreement's implied cooperation obligations.
How to Reclaim Authority When Staff Still Defer to the Seller
The contract is clear. The seller's role is patient introductions only. But your office manager still asks him whether she can approve PTO requests. Your lead hygienist checks with him before ordering supplies. Your front desk defers to his preferences when blocking your schedule. The problem isn't that the seller is actively undermining you — it's that staff hasn't internalized the power shift yet, and every time they go to him with a question, your authority erodes.
The First 30 Days Set the Pattern
The initial weeks after acquisition are when staff form their perception of leadership, and if the seller continues answering operational questions during that window, the team learns that real decisions still flow through him. It doesn't matter that you're signing the checks — symbolic authority is what staff respond to, and the seller holds it until you actively take it.
Pay attention to how staff phrase questions. If they're asking you "Is it okay if I..." but asking the seller "What should I do about...", they're treating you as permission-granter and him as decision-maker. That distinction matters. The first framing assumes you'll approve what they've already decided. The second assumes he'll tell them what to decide. You want staff coming to you with the second type of question.
Script the Seller's Response
The fastest way to transfer authority is to control what the seller says when staff approach him. Before the transition starts, have a direct conversation: "When staff come to you with questions about scheduling, supplies, or operations, I need you to redirect them to me. The exact words matter — I'd like you to say, 'That's Dr. [Buyer]'s call now. Check with them.'"
This isn't about embarrassing the seller — it's about creating a consistent message that reinforces the new structure. If the seller answers some questions and deflects others, staff will keep testing to see which category each issue falls into. If he deflects every time, they'll stop asking within a week.
Where this breaks down is when the seller adds qualifiers: "Well, I used to handle it this way, but you should check with Dr. [Buyer]." That sounds helpful but signals his way was the right way and you're the variable. A cleaner redirect — "That's not my decision anymore" — removes the implicit comparison and makes the authority transfer unambiguous.
Hold a Joint Handoff Meeting in the First Week
The single most effective tool for establishing authority is a staff meeting where the seller explicitly transfers decision-making power in front of the entire team. This isn't a casual introduction — it's a scripted moment where the seller says clearly: "As of today, Dr. [Buyer] is running the practice. All operational decisions go through them. If you have questions about scheduling, supplies, protocols, or anything else, bring them to Dr. [Buyer]. I'm here to help with patient introductions, but I'm not involved in day-to-day operations anymore."
The meeting should happen within the first three business days after closing. Waiting two weeks gives staff time to fall back into old patterns. The seller's tone matters as much as the words — if he sounds reluctant or frames it as temporary ("while I'm stepping back"), staff will interpret it as a trial period rather than permanent shift.
After the seller speaks, you reinforce: "I'm excited to be here, and I want to make sure you feel supported during this transition. If something comes up and you're not sure who to ask, the answer is me. I'll rely on [seller's name] for patient introductions and clinical handoffs, but everything else runs through me now."
Identify Who's Most Attached to the Seller
Not all staff members transfer loyalty at the same speed. Some adapt within days. Others need weeks of consistent reinforcement before they stop reflexively checking with the seller. A smaller subset will struggle to adjust at all — either because they're deeply loyal to the seller personally or uncomfortable with change.
Long-tenured employees often have the hardest time adjusting to new leadership, not because they're resistant but because their entire professional identity is tied to the old structure. Your office manager who's been there 15 years isn't just losing a boss — she's losing the person who taught her the job, trusted her with responsibility, and validated her expertise.
For those staff members, extra reassurance helps. Pull them aside individually in the first week: "I know this is a big change, and I want you to know I value the experience you bring. I'm not here to undo what's working — I'm here to build on it. If something feels off or you're not sure how I want something handled, just ask."
The harder case is the staff member who actively resists the authority transfer — who continues going to the seller even after he's redirected them, who undermines your decisions in front of patients, or who frames every change as a step backward. That's not a transition challenge — that's a retention risk. If someone can't accept that you're running the practice after 30 days of consistent messaging, they're unlikely to accept it after 90.
When to Address Overstepping Directly
Most sellers don't intend to interfere. They're responding to staff questions out of habit, offering input because they assume it's helpful, or weighing in on decisions because no one told them not to. But intent doesn't matter if the effect is the same: staff see the seller as the real authority, and you're left managing around him.
If the seller continues answering operational questions after you've scripted his redirect, or if he's contradicting your decisions in front of staff, you need a direct conversation. Framing it as alignment — "I want to make sure we're presenting a unified message to the team" — keeps the focus on the outcome rather than blame.
A structure that works: "I've noticed staff are still coming to you with questions about [specific examples]. I know you're trying to be helpful, but when you answer those questions, it creates confusion about who's making decisions. Going forward, I need you to redirect them to me every time, even if it feels awkward. That's the only way the team will internalize that I'm running the practice now."
Most sellers will course-correct once the issue is named clearly. If they don't — if they continue positioning themselves as the decision-maker after you've addressed it directly — that's when the early termination clause becomes relevant.
When to Cut the Transition Short and What Happens Next
The transition period has a defined end date, but that doesn't mean you're required to wait until day 90 to make a change. When the seller's presence costs you more authority than it provides continuity, ending the arrangement early isn't a failure — it's a business decision.
Three Signals the Transition Isn't Working
The clearest indicator the seller needs to leave is when staff behavior hasn't shifted after 30 days of consistent messaging. If your office manager is still seeking the seller's approval before implementing schedule changes, if your hygienists are checking with him before ordering supplies, or if your front desk is deferring to his preferences when patients call, the transition structure has failed.
A second pattern is when the seller contradicts your directives in front of staff or patients. This doesn't always look like open conflict. Sometimes it's subtle: you implement a new protocol, and the seller mentions to a staff member that "we never needed that before." You adjust the schedule template, and the seller tells the front desk that "the old system worked fine." Each instance is small, but the cumulative effect is that staff see your decisions as optional and the seller's preferences as baseline. When a seller continues to exert influence over operations after the sale, it can constitute interference with the buyer's business relationships.
The third signal is patient confusion. If patients are still asking when "Dr. [Seller]" will be back full-time, or if they're expressing concern that "things are changing too fast," the seller hasn't positioned you as the permanent owner.
Check Your Agreement for Early Termination Language
Before you initiate a conversation about ending the transition early, review your purchase agreement. Some agreements include an explicit early termination clause that allows either party to end the arrangement with 7–14 days' notice. If that language exists, you have a straightforward path: provide written notice, fulfill any remaining compensation obligations for the notice period, and move forward.
If the agreement doesn't include early termination language, you'll need to negotiate the exit rather than invoke a contractual right. Most sellers who are interfering are also uncomfortable with the new dynamic. They're fielding questions they don't want to answer, navigating a power structure that no longer includes them, and watching someone else run the practice they built. In many cases, they're relieved when the buyer suggests an early exit, especially if it's framed as a mutual decision rather than termination.
One approach that works: "I think we've accomplished what we needed to with the transition, and I don't want to keep you here longer than necessary. What if we wrapped up at the end of this week instead of continuing through [original end date]? I'll make sure you're compensated through Friday, and we can position it to the team as an accelerated handoff."
Document Specific Instances Before You Act
If the seller is actively undermining your authority and you anticipate resistance to an early exit, documentation matters. Before you raise the issue, create a written record of specific instances where the seller overstepped: dates, witnesses, and the impact on your ability to manage the practice.
What to document: times the seller contradicted your decisions in front of staff, instances where he answered operational questions after being asked to redirect them, and any situations where he positioned himself as the decision-maker to patients. Email yourself a summary after each incident so you have a timestamped record. If the seller's behavior crosses into interference with your business relationships or violates the non-compete provisions, that documentation becomes the foundation for enforcement.
Communicate the Early Exit as an Accelerated Transition
How you explain the seller's departure to staff and patients determines whether it destabilizes the practice or reinforces your authority. Position it as a planned acceleration: "Dr. [Seller] and I agreed that the transition has gone smoothly, and we're ready to move to the next phase sooner than we originally planned. His last day will be [date], and I'm excited to continue building on the foundation he created."
For patients, the message is simpler: "Dr. [Seller] has fully transitioned out of the practice as planned. I'm grateful for his help during the handoff, and I'm looking forward to continuing your care." Most patients won't ask follow-up questions if the message is confident and forward-looking.
What to Do If the Seller Won't Leave After the Transition Period Ends
The harder scenario is when the transition period expires but the seller continues interfering — not by showing up to the office, but by contacting staff, reaching out to patients, or undermining your reputation in the community. At that point, the issue isn't transition friction — it's whether the seller is violating the non-compete or non-solicitation provisions of your purchase agreement.
If the seller is actively soliciting patients or encouraging staff to leave, that may constitute tortious interference or breach of contract. The first step is a cease-and-desist letter from your attorney, outlining the specific behavior and the contractual provisions it violates. Most sellers stop once they receive formal legal notice.
If the behavior continues, you'll need to decide whether enforcement is worth the cost. Litigation is expensive, and even if you win, the reputational damage of a public dispute with the previous owner can linger. A more practical path in some cases is to focus on rebuilding patient and staff confidence rather than pursuing legal action.
The transition period is temporary, but the authority you establish during it isn't. If the seller's presence is preventing you from taking control of the practice you bought, ending the arrangement early isn't a sign of failure — it's a recognition that the cost of waiting has started to exceed the benefit of continuity.
Sources & References
The data and claims in this article are drawn from the following sources. We prioritize government data, peer-reviewed research, and established industry publications to ensure accuracy.
- 4 Common Dental Practice Transition Mistakes and How to Avoid ...— practicefinancialgroup.comIndustry
- How to Manage Founder Transition After Acquisition | Izba— izba.coIndustry
- The Dental Practice Transition Period— www.adstransitions.comIndustry
- Transition/Consulting Agreements After the Sale of a Business— vennlawgroup.comIndustry
- Transfer of authority in the dental practice: Buyer vs. Seller— www.dentistryiq.comIndustry
- When is it Improper for the Seller of a Business to Solicit his Former ...— www.mccmlaw.comIndustry
- How to Handle Disputes with the Previous Owner of a Dental Practice— www.dmcounsel.comIndustry
Frequently Asked Questions
Navigate seller transitions with expert guidance
Post-closing complications require experienced support. Minty Plus provides hands-on practice management assistance to help you establish independence and resolve transition challenges after your acquisition.


