Incomplete Patient Records in Dental Practice Due Diligence
Co-Founder, Minty Dental

In Summary
- Missing treatment notes, outdated medical histories, and gaps in radiographic documentation expose compliance risk under HIPAA, inflate active patient counts, and make revenue projections unreliable
- Systematic gaps across all charts typically indicate broken operational systems, while selective gaps in high-value treatment areas may signal intentional documentation avoidance
- Practices with strong documentation quality tend to have better systems overall—making chart quality a reliable proxy for operational health
- The ADA's documentation standards provide a baseline for complete records: medical histories, treatment notes, radiographs, consent forms, and billing documentation
- Recent improvements in documentation quality right before a sale often indicate pre-sale cleanup rather than sustained operational discipline
Incomplete Records Signal More Than Poor Documentation
When you pull a random sample of patient charts during due diligence, you're diagnosing the operational health of the practice you're considering buying. Missing treatment notes, outdated medical histories, gaps in radiographic documentation, and absent consent forms reveal how the practice has been managed—and what risks you're inheriting.
The ADA's documentation standards establish what complete patient records should contain: personal data, medical and dental histories with updates, progress and treatment notes, diagnostic records including radiographs, medication prescriptions, informed consent forms, and documentation of treatment discussions.
Documentation gaps create three immediate threats to deal value. First, they expose you to compliance risk under HIPAA and state regulations—incomplete records make it nearly impossible to demonstrate you're meeting standards of care or maintaining required patient privacy protections. Second, they inflate active patient counts when charts haven't been properly archived or updated, making the patient base look larger and more valuable than it actually is. Third, they make revenue projections unreliable when treatment history is unclear or billing records are incomplete. One protection many buyers overlook is asking specific questions about documentation practices before the LOI stage, when you still have leverage to walk away cleanly.
The pattern of incompleteness tells you what's broken. Systematic gaps across all charts—missing medical history updates, absent radiographs, incomplete treatment notes—suggest broken systems or high staff turnover. Selective gaps in high-value treatment areas may indicate documentation avoidance, where providers skip notes on complex cases to reduce liability exposure or avoid scrutiny. Recent documentation improvements right before listing often signal pre-sale cleanup rather than sustained operational discipline.
Practices that audit their records regularly tend to have stronger systems overall—better compliance protocols, lower risk exposure, and more accurate financial reporting. Chart quality correlates directly with operational health because documentation discipline requires functional systems, trained staff, and consistent oversight. When you find clean, complete records, you're usually looking at a practice where other operational details are also managed well. This is one reason buyers often miss critical operational issues during evaluation—they treat documentation as a separate compliance concern rather than a diagnostic tool for the entire operation.
How to Conduct a Patient Chart Audit That Actually Works
Most buyers approach chart audits as a compliance checkbox—pull a few files, confirm they exist, move on. That approach misses the point. A systematic audit tells you whether the patient base is real, whether the revenue is sustainable, and whether you're inheriting operational discipline or operational debt.
Start by determining your sample size and selection criteria. Industry practice suggests reviewing 50-100 charts representing different patient segments: new patients from the past 12 months, recall patients with multiple visits over several years, and treatment patients with recent complex procedures. Stratify your sample across time periods—pull charts from 6 months ago, 18 months ago, and 3 years ago to see whether documentation quality has been consistent or has degraded over time.
For each chart, examine five core elements:
Medical history completeness and update frequency — Look for initial intake forms, annual updates, and documentation of changes when patients return after gaps
Treatment note quality and timeliness — Notes should be entered the same day as treatment, include specific details about procedures performed, and support the codes billed
Consent form presence for major procedures — Endodontics, extractions, periodontal surgery, and cosmetic work should all have signed consent documentation
Radiograph documentation and quality — Verify that diagnostic images exist, are dated correctly, and match what treatment notes describe
Alignment between clinical notes and billing codes — When a chart shows a crown prep but billing shows a simple restoration, you've found either coding errors or documentation gaps that inflate reported production
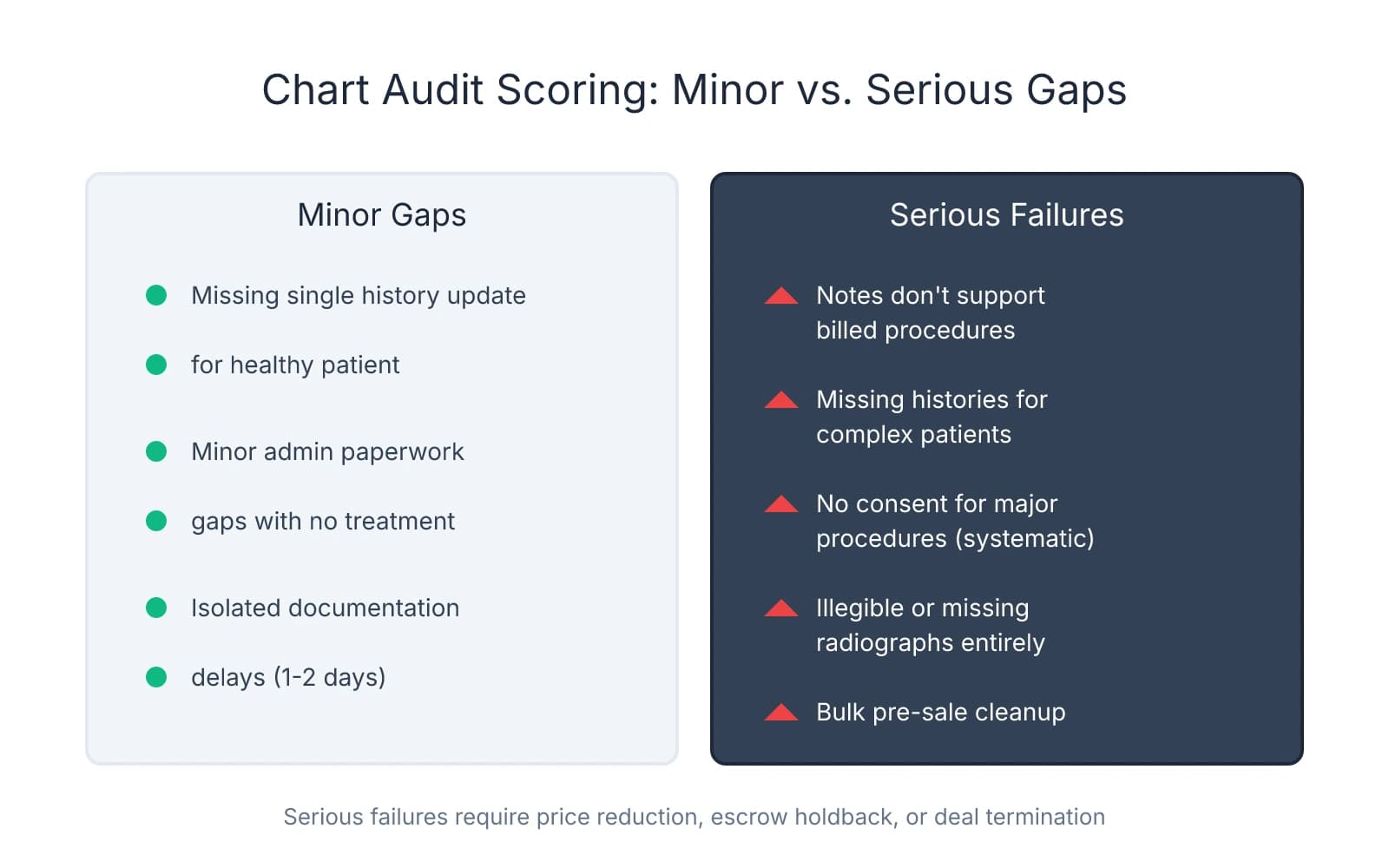
Create a scoring rubric that distinguishes minor administrative gaps from serious compliance failures. Minor gaps might include missing a single medical history update for a healthy patient with no treatment in that period. Serious failures include treatment notes that don't support billed procedures, missing or outdated medical histories for patients with complex conditions like diabetes or anticoagulant use, systematic absence of informed consent across multiple major procedures, and radiographs that are illegible or missing entirely for diagnosed treatment. Calculate an overall documentation quality score by assigning point values to each element and averaging across your sample—this gives you a quantifiable metric to reference in negotiations.
Chart audits typically occur after LOI signing during the due diligence period, when you have contractual access to records but before you've committed to final terms. Plan for 1-2 days of on-site access, ideally with someone who has clinical knowledge and can assess whether documentation meets standards of care—not just whether forms exist. Some buyers bring in consultants for objectivity, particularly when they lack experience evaluating documentation quality or want an independent assessment they can cite in negotiations.
Document your findings in a structured format that supports negotiation leverage. Create a summary table showing the percentage of charts with complete documentation, the percentage with minor gaps, and the percentage with serious compliance issues. Include specific examples of problematic charts with patient identifiers removed—these concrete cases carry more weight than general observations. If your audit reveals that 40% of charts are missing informed consent for major procedures, that's not a minor paperwork issue—it's a compliance liability that should adjust either the purchase price or the terms of your indemnification clause.
Watch for red flags that should trigger deeper investigation. Recent bulk documentation that suggests pre-sale cleanup—like 200 medical history updates all dated within the same week—indicates the seller is aware of gaps and scrambling to fix them before you look. Treatment notes that consistently don't support billed procedures suggest either systematic upcoding or documentation shortcuts that create audit risk. Missing or outdated medical histories for patients with complex conditions expose you to malpractice liability if something goes wrong post-transition and you can't demonstrate you knew about their health status.
The audit isn't just about finding problems—it's about understanding what you're buying and structuring protections accordingly. Clean charts with minor gaps might justify a standard indemnification clause. Systematic documentation failures might justify a purchase price reduction, an escrow holdback for compliance remediation, or walking away entirely if the risk is too high to manage.
What Incomplete Records Mean for Active Patient Count and Revenue
Documentation quality directly determines whether the two numbers driving your valuation—active patient count and sustainable revenue—are real or inflated. When charts are incomplete, you can't verify that the seller's claimed 1,500 active patients actually represent 1,500 people who will return for care.
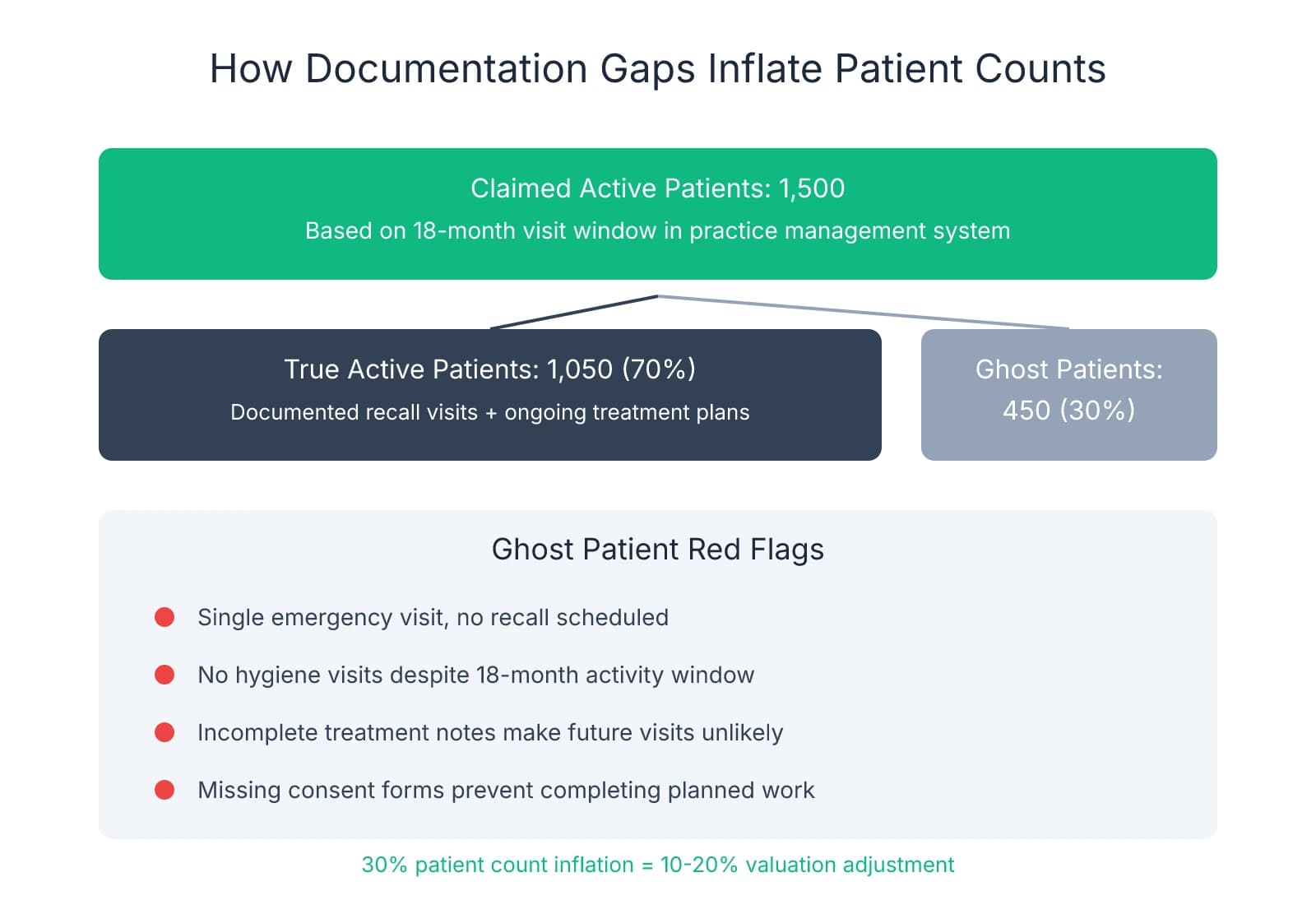
The active patient count problem starts with definition ambiguity. Most practices define "active" as any patient seen within 18 months, but incomplete records make it impossible to distinguish truly active patients from one-time emergency visits that will never convert to ongoing care. A chart with a single emergency extraction from 14 months ago counts as "active" in the practice management system, but that patient has no recall appointment scheduled, no treatment plan on file, and no documented follow-up. When 20-30% of your claimed active base fits this pattern, you're not buying 1,500 patients—you're buying 1,050 patients plus 450 ghosts who inflate the numbers but won't generate future revenue.
Missing recall documentation compounds this problem. If charts don't show consistent hygiene visits, you can't verify patient loyalty or predict future retention. A patient seen twice in 18 months for restorative work but never for hygiene may be practice-hopping for specific procedures rather than establishing a long-term relationship with the practice.
Incomplete records create three specific revenue risks:
Incomplete treatment notes make it impossible to assess the value of unscheduled treatment — When the seller claims $200K in treatment planned but not yet completed, you need detailed notes showing what was diagnosed, what was presented to the patient, and why it wasn't scheduled
Missing consent forms may legally prevent you from completing planned high-value procedures — If a patient was diagnosed for a crown but there's no signed consent form documenting the discussion, you may need to restart the treatment planning process entirely—which gives the patient an opportunity to decline or seek care elsewhere
Inadequate documentation increases the risk of insurance audits and clawbacks — When treatment notes don't support the codes billed, insurers can demand repayment for procedures they consider improperly documented—and those clawback demands typically arrive 12-18 months post-transition, when you own the liability but the seller has moved on
Where buyers often get burned is treating documentation gaps as a separate compliance issue rather than a valuation issue. When your chart audit reveals that 40% of charts have incomplete treatment notes and 30% are missing consent forms for major procedures, that's evidence that the practice's stated active patient count and revenue projections may be overstated by 20-30%. One protection many buyers find valuable is calculating a documentation discount that adjusts the purchase price to reflect this uncertainty. If the seller is asking for 75% of collections based on a claimed 1,500 active patients, but your audit suggests only 1,050 of those patients have documentation supporting ongoing care, you're justified in reducing the price by 10-20% or structuring an earnout that pays the seller only after you verify patient retention and revenue sustainability over 12-24 months.
Use your chart audit findings as negotiation leverage by presenting specific documentation gaps as evidence that the numbers don't hold up. Instead of making general statements about poor record-keeping, show the seller a table: "Of the 100 charts we reviewed, 35 had no documented hygiene visit in the past 18 months, 28 had incomplete treatment notes that don't support billed procedures, and 22 had no consent forms for major procedures completed in the past year. Based on this sample, we estimate that 30-40% of your claimed active patient base either won't return or represents compliance liability we're inheriting."
When documentation quality is questionable, structure deal protections that transfer risk back to the seller. An earnout tied to patient retention—where the seller receives 20-30% of the purchase price only if 80% of active patients return within 12 months—aligns incentives and ensures you're paying for real patients, not inflated counts. Enhanced seller warranties that require the seller to indemnify you for insurance clawbacks resulting from pre-transition documentation failures protect you from audit risk you can't fully assess during due diligence. An escrow holdback of 10-15% of the purchase price for 18-24 months gives you a financial cushion if revenue drops because the patient base wasn't as strong as represented.
The pattern worth paying attention to: practices where seller production props up revenue almost always have documentation gaps that make it impossible to verify whether patients are loyal to the practice or loyal to the seller. When the seller is the primary producer and documentation is weak, you're buying a patient base that may evaporate the moment the seller leaves—and you won't know until it's too late to adjust the deal terms.
Structuring Deal Protections When Records Are Incomplete
When your chart audit reveals documentation gaps, the question isn't whether to proceed—it's how to structure protections that shift risk back to the seller and give you recourse if problems surface after closing.
Start with seller representations and warranties that create explicit accountability for record quality. Request language stating that all patient records are complete, accurate, and compliant with state and federal requirements—not just that they exist. Require the seller to warrant that the active patient count is based on patients seen within 18 months with complete documentation supporting ongoing care, not just system-generated reports that include one-time emergency visits. Include a warranty that there are no pending or threatened compliance audits, insurance investigations, or documentation-related disputes.
Indemnification provisions determine who pays when documentation failures create financial consequences. Require the seller to indemnify you for losses resulting from incomplete records—including insurance clawbacks when treatment notes don't support billed codes, regulatory penalties if state board audits find documentation deficiencies, and malpractice claims arising from inadequate documentation of the seller's treatment decisions. Standard indemnification clauses often include caps and baskets that limit the seller's exposure, but when documentation quality is questionable, negotiate for higher caps or carve-outs that exclude documentation-related claims from the cap entirely.
Escrow holdbacks and earnout structures give you leverage when documentation quality makes revenue sustainability uncertain. Hold back 10-20% of the purchase price in escrow for 12-18 months to cover documentation-related claims—this creates a financial cushion you can draw against if insurance audits result in clawbacks or if patient retention drops because the active count was inflated. Alternatively, structure an earnout that pays the seller only after you verify patient retention and revenue sustainability over 12-24 months.
HIPAA transfer requirements and record access protections ensure you can defend yourself if documentation problems lead to legal or regulatory challenges. The purchase agreement should include language requiring the seller to maintain records for the statutory retention period—typically 7-10 years depending on state law—and to provide you access for malpractice defense or regulatory response. Confirm that patient notification letters will be sent announcing the ownership change and that the seller will cooperate with any records requests that arise post-transition.
Where many buyers get burned is accepting generic indemnification language that sounds protective but includes caps, baskets, and time limits that make it nearly impossible to recover losses. A clause that limits the seller's liability to 10% of the purchase price with a $25,000 basket and an 18-month survival period may sound reasonable—until you discover that an insurance audit results in $150,000 in clawbacks 20 months after closing. When documentation quality is questionable, negotiate for terms that reflect the actual risk: longer survival periods for documentation-related claims, higher or eliminated caps, and lower baskets that don't require you to absorb the first $25,000 in losses before indemnification kicks in.
One decision framework that helps clarify when to walk away: if more than 30% of sampled charts have serious documentation gaps—missing consent forms for major procedures, treatment notes that don't support billed codes, or systematically absent medical histories for complex patients—the compliance risk may outweigh the opportunity. If the seller refuses to provide access for a proper audit or becomes defensive when you raise documentation concerns, that's a signal they know the records are worse than disclosed and are hoping you won't look closely.
Walking away from a deal is sometimes the right call when the documentation risk is too high to manage through contractual protections alone. But when gaps are moderate and the seller is willing to negotiate, the right combination of warranties, indemnification, escrow holdbacks, and earnouts can turn documentation uncertainty into a structured risk you can manage—rather than an open-ended liability that haunts you for years after closing.
Sources & References
The data and claims in this article are drawn from the following sources. We prioritize government data, peer-reviewed research, and established industry publications to ensure accuracy.
- What to Do with Patient Records When Selling a Practice— ada.orgIndustry
- A Case for Auditing Your Dental Records— dentalcompliance.comIndustry
- Conducting Due Diligence When Buying a Practice— watsonbrownsales.comIndustry
- Patient Record Audit: Suggestions for Buyers - OMNI Practice Group— omni-pg.comIndustry
- [PDF] The Most Important Number– The Active Patient Count - Henry Schein— henryschein.com
- Handle With Care: Protecting Patient Records Upon Sale of a Dental ...— ddslawyers.com
Frequently Asked Questions
Ensure Complete Records Before Buying
Thorough due diligence on patient records is critical when acquiring a dental practice. Minty Plus provides expert guidance through every step of the acquisition process, including comprehensive chart audits and documentation verification.


